All content on this site is intended for healthcare professionals only. By acknowledging this message and accessing the information on this website you are confirming that you are a Healthcare Professional. If you are a patient or carer, please visit the Lymphoma Coalition.
The lym Hub website uses a third-party service provided by Google that dynamically translates web content. Translations are machine generated, so may not be an exact or complete translation, and the lym Hub cannot guarantee the accuracy of translated content. The lym and its employees will not be liable for any direct, indirect, or consequential damages (even if foreseeable) resulting from use of the Google Translate feature. For further support with Google Translate, visit Google Translate Help.


Now you can support HCPs in making informed decisions for their patients
Your contribution helps us continuously deliver expertly curated content to HCPs worldwide. You will also have the opportunity to make a content suggestion for consideration and receive updates on the impact contributions are making to our content.
Find out more
Create an account and access these new features:
Bookmark content to read later
Select your specific areas of interest
View lymphoma & CLL content recommended for you
EHA-SWG 2017 | Rare Lymphomas: Treatment of WM
On March 11th, at the EHA-SWG Rare Lymphomas Scientific Meeting 2017 in Barcelona, Spain, Marie José Kersten chaired a scientific session on ‘Waldenström’s Macroglobulinemia’. The second presentation of this session was originally intended to be presented by Meletios Dimopoulos, but was presented by Marie José Kersten on the topic of ‘Treatment of WM’. Below are the key highlights from this presentation:
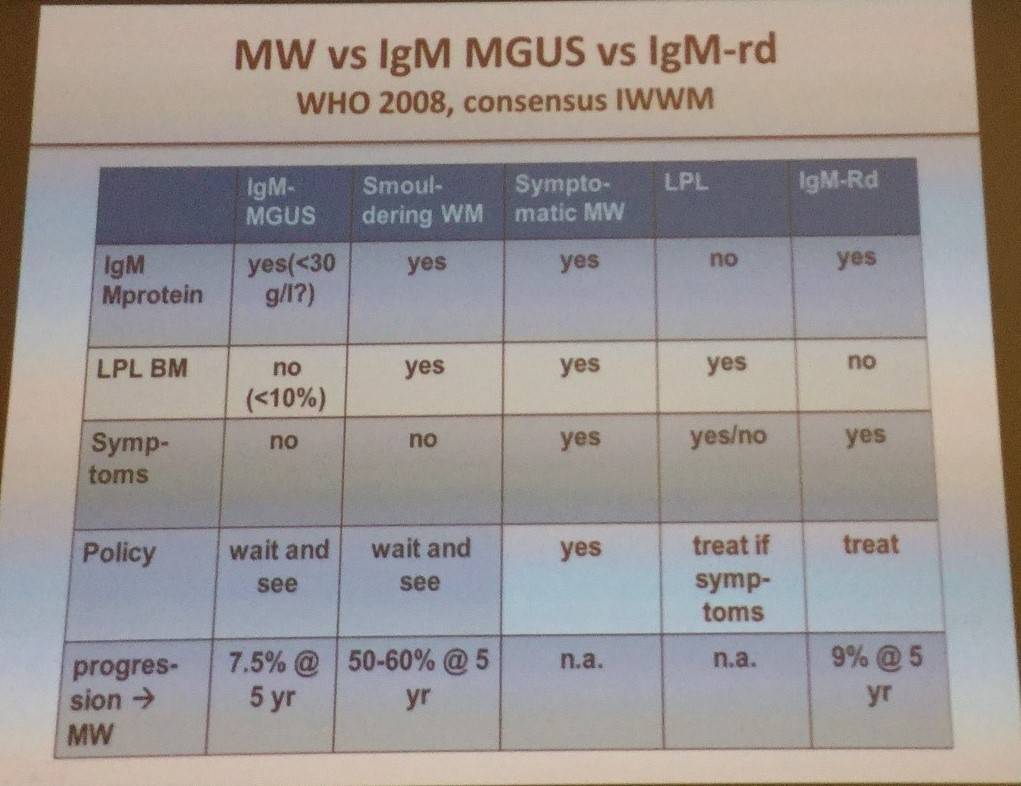
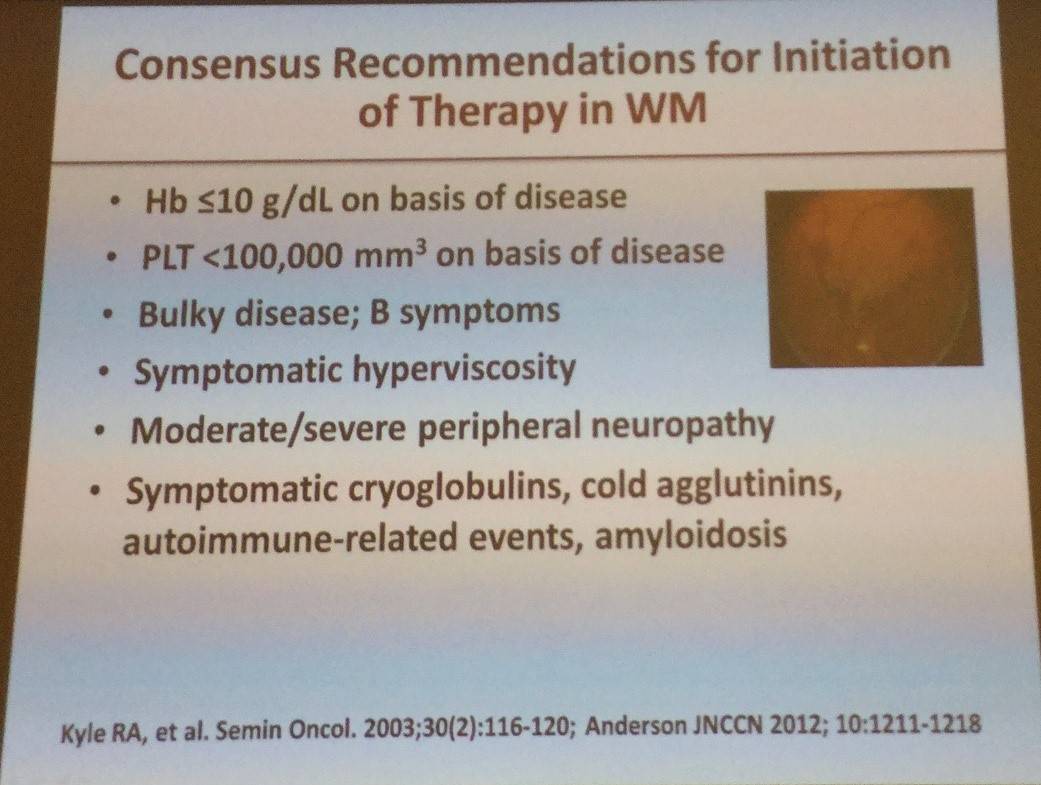
- The session began with an overview of WM and when to initiate therapy
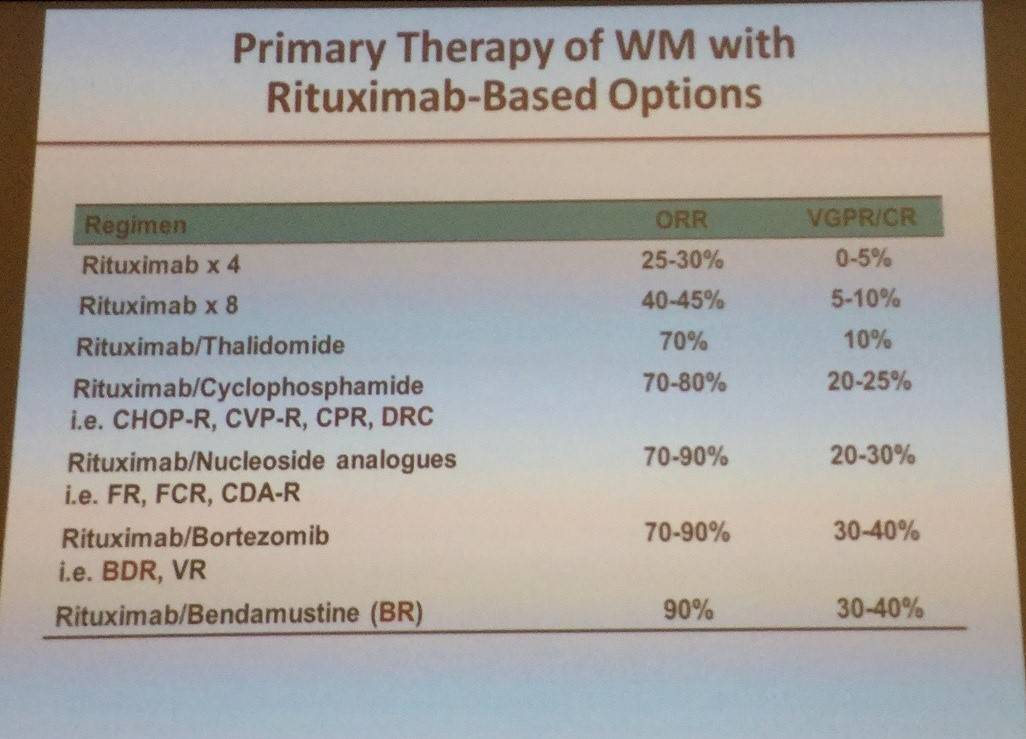
- Options for treating WM have expanded greatly in the last decade and now include proteasome inhibitors, rituximab, alkylating agents, monoclonal antibodies, etc.
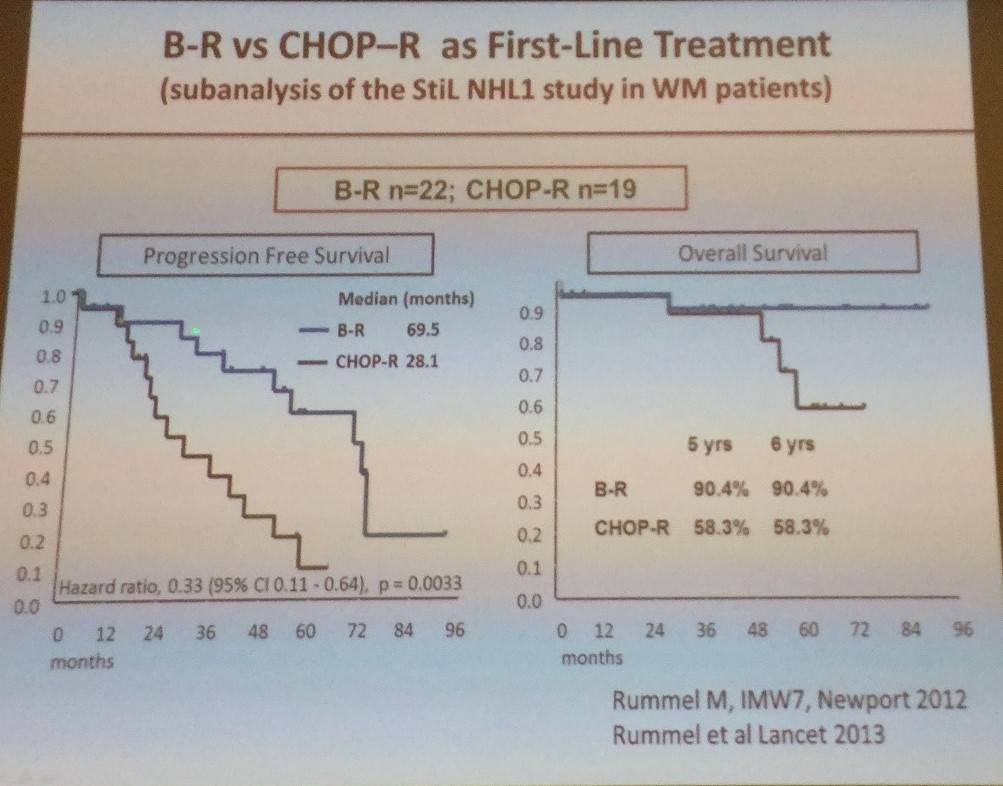
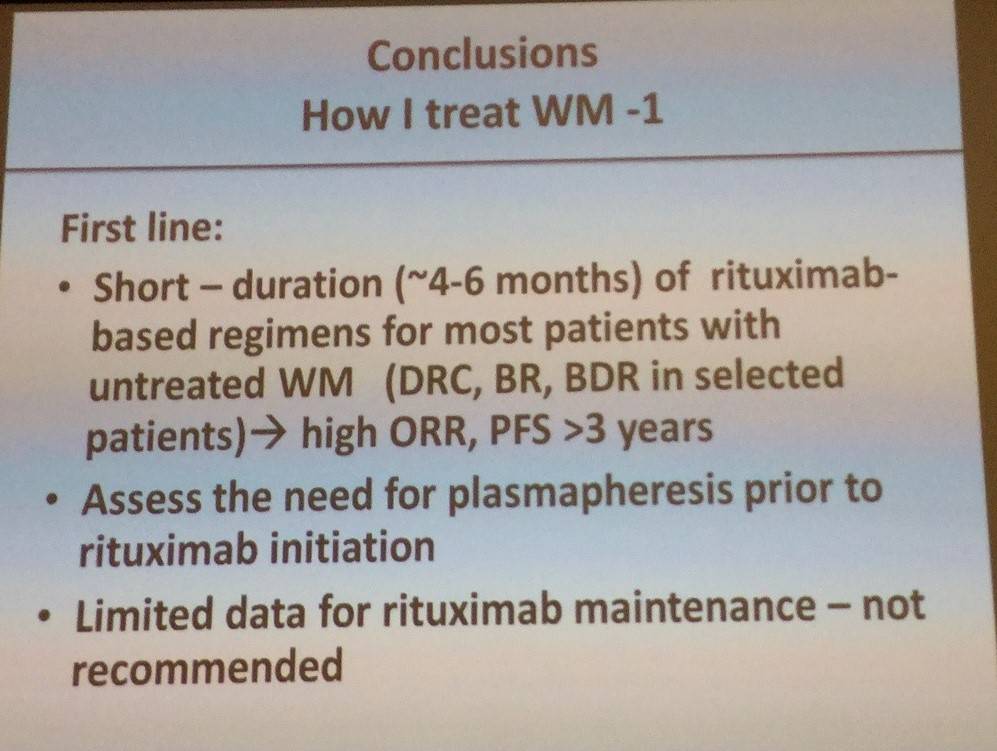
- Rituximab-based regimens have the best outcome for first-line WM patients
- Dexamethasone, rituximab, cyclophosphamide treatment was shown to have 83% ORR. But with high IgM flare rate (32% pts; 11% pts >25% IgM increase)
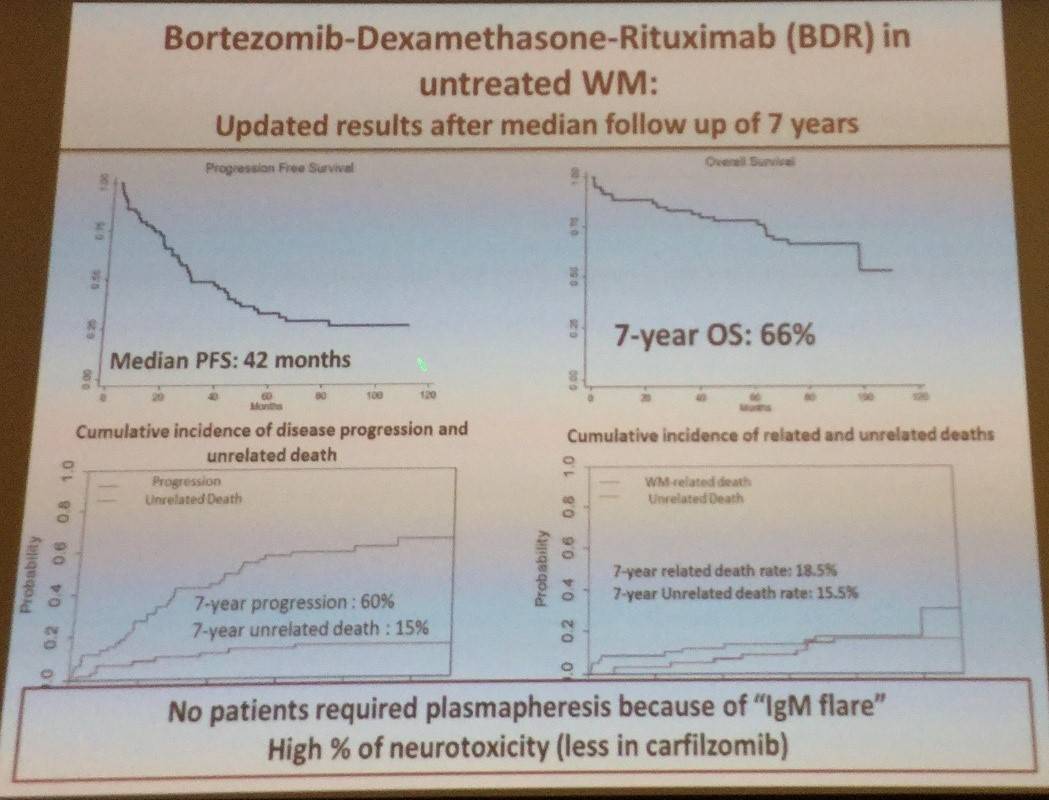
- A summary of data for proteasome inhibitors and combination therapy was presented, and it was reported that no pts needed plasmapheresis due to IgM flare:
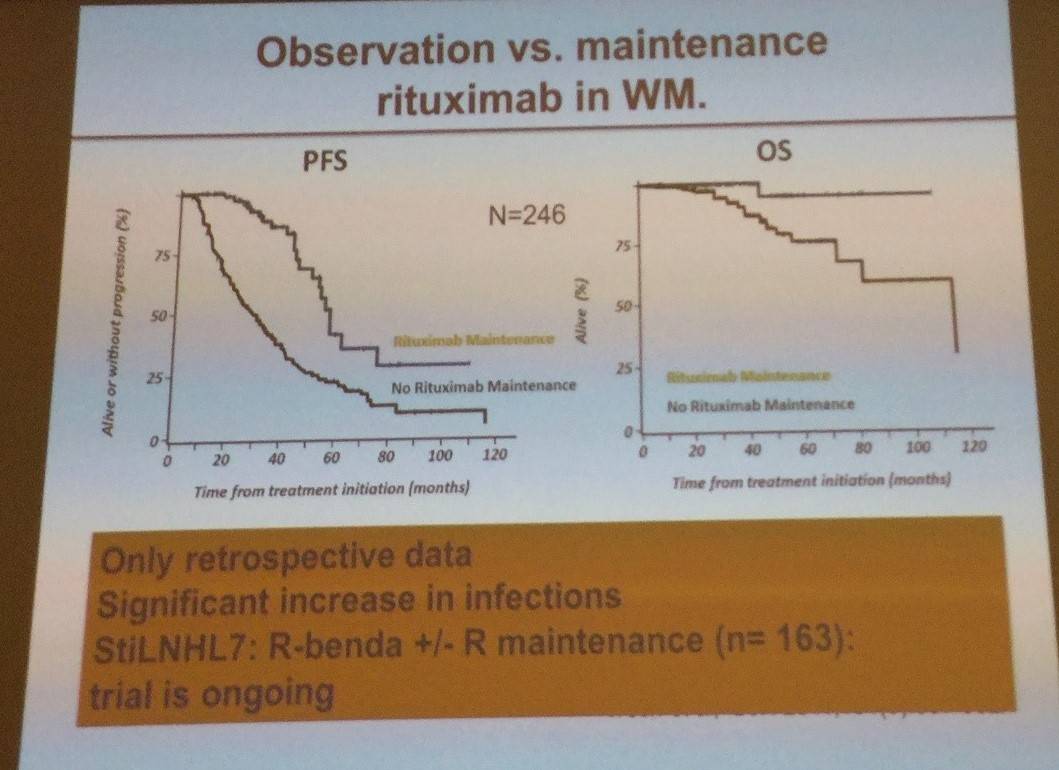
- Rituximab maintenance was shown to result in significantly higher PFS and OS in patients with WM however, this data was from a retrospective analysis
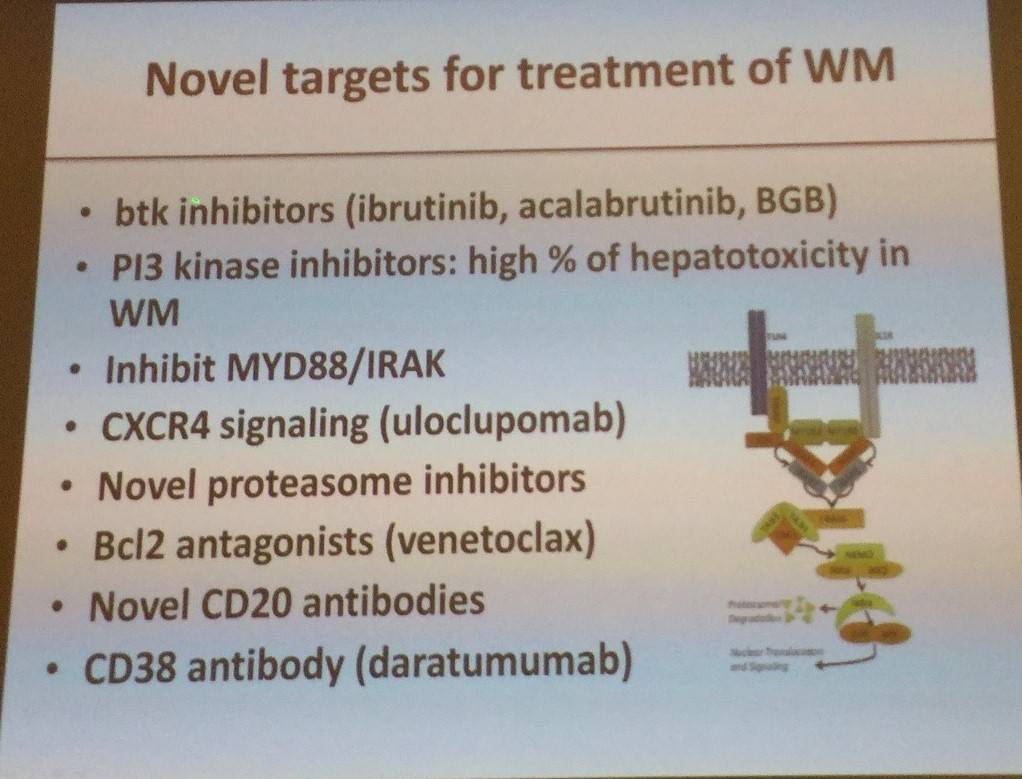
- Novel drug targets:
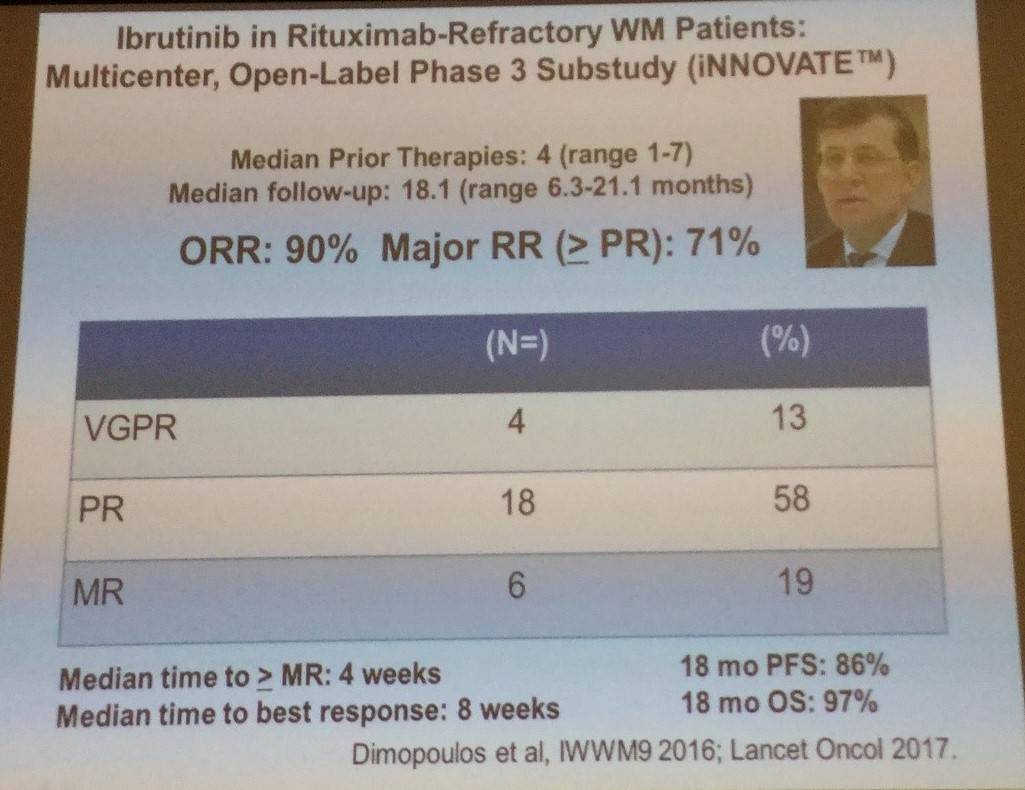
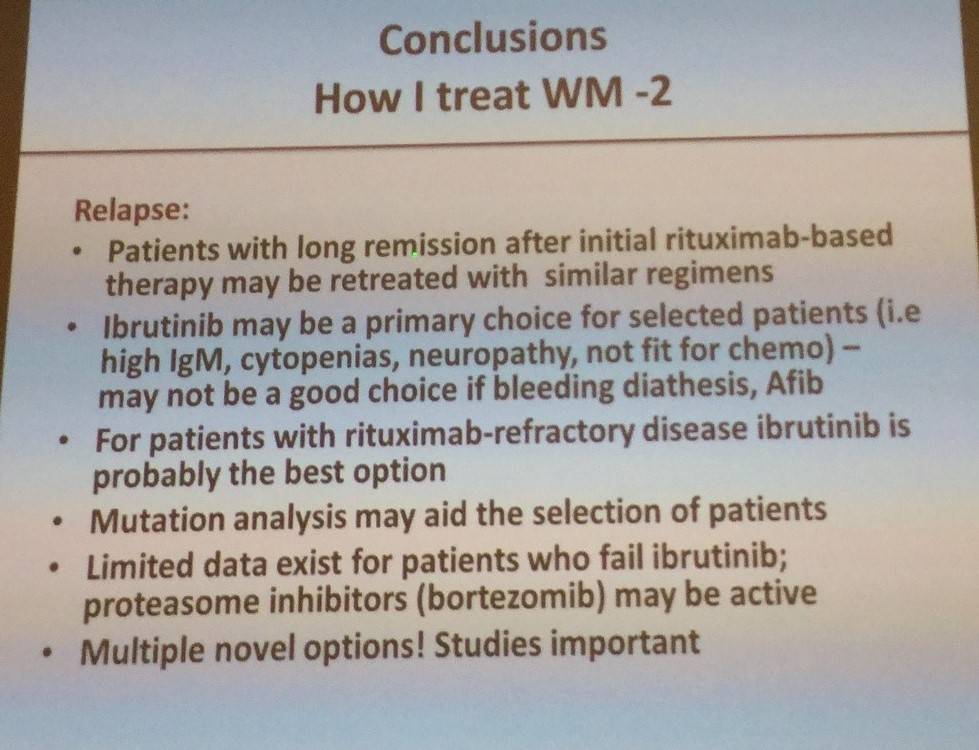
- Ibrutinib has been shown to be effective in previously treated WM with a 68.1% EFS (95% CI), 90% OS (95% CI) with a median follow-up of 37 months
- In conclusion, rituximab-based therapy is recommended in first-line patients, but evidence is less clear for relapsed WM patients
References